So while my layman's research/experience may be helpful/informative, please consult a medical professional for your personal situation.
Scroll down for full details, but since the 2011 surgery, I continue to see well and am glad with the choices I made and the results.
Around age 40, it slowly started becoming more difficult to focus (when wearing correction) at close distances, especially in low light. This is a very common condition called Presbyopia which is due to your crystalline lens becoming less elastic. This loss of accommodation is analogous to camera lens that won't focus close. So I started wearing reading glasses (when wearing contacts) or a different glasses prescription for computer/close-in work. Wendy made fun of me, but I said "wait until your turn" and yes, a few years later, she had to start wearing reading glasses - her distance vision remains excellent.
In 2010 (age 46), I noticed that my right eye had more difficulty seeing things. I had been told it had a "small" cataract, but these can often exist for years with no impairment of vision. Unfortunately, I had a Posterior Subcapsular Cataract - these "grow" faster, are more prevalent in younger people, and cause greater visual degradation due to the location at the rear of the visual axis. Because of the cloudiness, you are no longer able to correct to 20-20. An analogy would be a blown window that now has a permanent haze. In addition, the cataract causes a "Myopic Shift" which means increased spherical power (also noticeable via reduced minimum focusing distance) and astigmatism - i.e. a new pair of glasses/contacts every several months which is a bit of a PIA. Cataracts typically don't interfere with vision and lifestyle until age 70 or later ... so it kinda sucks to have it happen to me a few decades early - darn!
I'm a bit of a photographer who analyzes camera gear (and shoots with my right eye - bummer!), so I'm aware that image quality encompasses more than just seeing "20-20" on the eye chart. For instance, I check the MTF curves and will often see various visual defects in my pictures such as Chromatic Aberration that might not be apparent to others - sometimes it's not good to know more. Being an Engineer, I'd periodically "test" my vision and needless to say, even pre-Cataract, I knew it wasn't sharp as it could be, but you just have to manage with the eyes you get.
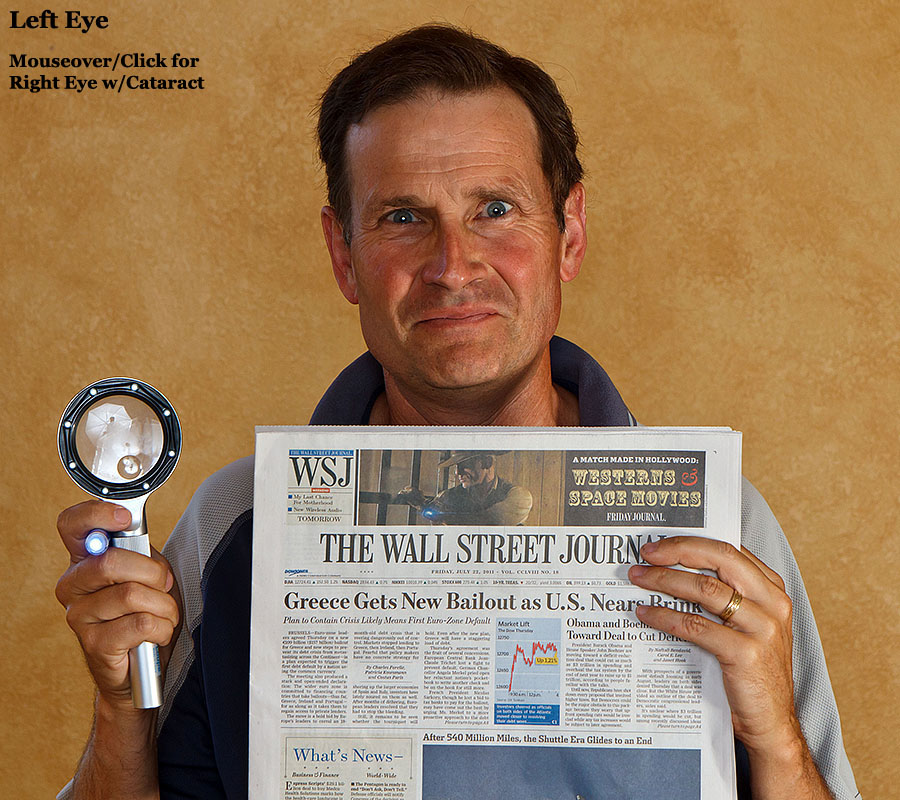
Even with best correction, the cataract impairs the vision and causes all sort of visual aberrations beyond just blurriness due to the cloudy lens. Point sources of light are "replicated" (as seen below) and high-contrast or low-light situations are difficult. Interesting enough (to me at least!) is that with one "good" and one "bad" eye, it's fairly easy for me to compare the visual degradation. It's amazing how the brain is able to "filter/figure" out the "bi-polar" vision (up to a point) but it requires a lot of "work" to see and I often get visual fatigue. Below is an image that simulates (as of July/2011) the difference I see between the left and right eye - HEY, less wrinkles with the later! ;-)
Image "flip" simulation of my vision clouded/defocused due to a cataract - NOT correctable with glasses
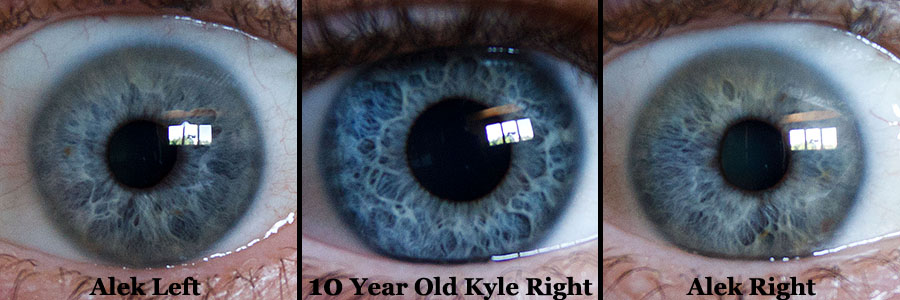
Alek's Left/Right Eye and 10-year old Kyle's right Eye ... all non-dilated and lit from windows
But recall that accommodation (or focus) is done by your eye's Ciliary muscles moving your natural lens ... which has now been replaced. So until about 10 years ago, IOL's were "mono-focal" - i.e. you could see 20-20 distance, but had no ability to focus at Intermediate or Close-in. Therefore, you'd still need to wear glasses for reading, and the fuzziness at Intermediate distances would affect your day-to-day life.
In the last decade, two competing technologies have tried to address this shortcoming. Multi-Focal lens are basically concentric rings of far/close focus so two images are presented to the brain and it is able to "pick" the sharp one depending on if you are looking far or near. Advantages are that you have a good chance of seeing well at far and near. Disadvantages are that your Intermediate will be fuzzy, and high contrast situations can be difficult with halos and glare. As an engineer, this is obviously a compromise solution ... but if no perfect solution is available, one often uses what is available/works ... and Multi-Focals are commonly used today.
The other approach is Accommodating Lens which uses the eye's own Ciliary Muscles (which focus your natural lens) to change focus. Obviously this would be the "Holy Grail" of IOL's ... if it works. As of 2011, the Bausch and Lomb Crystalens is the only accommodating IOL to have FDA approval. There seems to be more variable results with the Crystalens, but ideally, you should end up with excellent vision at Far and Intermediate, but you almost certainly will need Reading Glasses for close-up work. I.e. If all goes well with the Crystalens, you will have at least a diopter of accommodation and be able to go glasses-free for most day-to-day life, but need glasses for reading. Because it's not a compromise solution, halo/glare is less of an issue and I would expect better low-light vision than multi-focals.
It's interesting talking to Eye Doctors as there definitely are Multi-Focal and Accommodating "camps" with both believing their solution is the best and the other is (basically) no good. So as a layman (or at best a eye-doctor-wanna-be), it's quite confusing who to believe and select an option. And what is really a bummer is that there is lots of research (and money!) in this area so even a couple of years from now, there probably will be other options. For example, Synchrony and Tetraflex are two lens awaiting FDA approval that claim greater accommodation. Femtosecond Lasers may soon be the new scalpel in eye surgery, offering more precision and consistent results.
My guess is that by time I'm 70 (when most people start to be affected by Cataracts), technology will progress such that Accommodating Lens with multiple diopters of accommodation (so you can see Far/Inter/Near) will probably be commonplace. In fact, it would not surprise me that (similar to Lasik), refractive Cataract Surgery becomes popular as an elective option to correct vision and address Presbyopia.
Note that you really do NOT want to remove an IOL after it has been in
your eye as the risk of complications goes way up ... so "upgrading" years
later would be difficult. But speaking from first-hand experience, the
degraded vision from the Cataract really affects your lifestyle (and it is
rapidly getting more annoying) so I'd like to do something about it rather
than wait for the "next great thing." People describe Cataract Surgery
as an incredibly positive life-changing experience ... lets hope that
is the case for me.
So what did I decide to do? Turns out that Dr. Don Keller (who you may
recall did my wife's Lasik) is huge fan of the Crystalens ... and was
actually the first Doctor in Colorado to use 'em. So he obviously has a lot of
experience doing them ... and while Cataract surgery is fairly routine, there
certainly is a skill/experience element involved. He also spent a lot of time
with me discussing the various pros/cons/aspects of Cataract Surgery.
I'm OK with wearing glasses for reading, but it would sure be nice to
see 20-20 (or better!) at Far/Intermediate for sports and normal day-to-day life ... and hopefully no halo/glare at night.
So Crystalens seems to be the right choice for me at this time.
Some additional concerns are that due to my high Myopia, I'll have an even higher risk of Retinal Detachment during my lifetime. Also, I will probably have Posterior Capsule Opacity (PCO) sometime soon after the operation, but this is fixable with a ND:YAG laser that basically burns a hole in the back of the bag to clear the visual axis. My astigmatism (pre-cataract) isn't too much, but am hoping that a Limbel Relaxing Incision (LBI) during the operation may be able to reduce most of this. Note that while a Lasik tune-up is possible afterwards, you can't do a "custom" job after the IOL is in place since it messes up the measurements. Also, if you have had Lasik BEFORE cataract surgery, it will make the IOL measurements more difficult ... so it is helpful to have your eye measurements before you had that done along with the parameters of the Lasik surgery. Exercising the eye muscles by reading afterwards is highly recommended to "get/tune" them back into shape with the new accommodating lens and may take several months.
I should add that while the cataract in the left eye is not interfering with my vision too much, with -7 diopters of correction, you really need to have both done to balance things ... plus in dry Colorado, there is no way I could wear contacts all day long, every day. So another decision will be whether to do a ~1 diopter offset in the other eye (i.e. like mono-vision) to provide better near vision ... but this gives up some clarity at distance along with depth perception. For similar reasons, I'll want to do the 2nd eye as soon as possible (one week) after the 1st eye.
Cataract Surgery is covered by insurance, but only for mono-focal lens.
The upcharge for premium lens (multi-focal or accommodating) is about
$2,000 an eye. This is in addition to insurance deductibles, so it's not
cheap ... but since I'm not even 50 yet (and hopefully have some good years
left in me), it would sure be nice to see well after a lifetime of vision issues ... so I plan to have it done after Labor Day, 2011.
Expectations:
While everyone wants 20-20 (or 20-10!) at Far/Inter/Near, that's not
realistic with today's technology and Dr. Keller thinks that
"20-functional" is quite doable.
A very successful outcome for me would
be sharp (good contrast with no halos, glare, etc.) 20-20 vision at
distance and intermediate to 1/2 meter ... i.e. would
be super to get a full 2 diopters of accommodation and he says my
high myopia may help in that area as the football'ness shape of the eye
provides more flexure on the IOL.
As noted before, there are risks with any surgery, but they are pretty low for Cataract surgery and obviously I hope none of the short or long term problems crop up for me. One thing I'll have to worry about for life is retinal detachment ... with high myopia and cataract surgery, it seems this happens to over 5% of people - not insignificant!
Cataract surgery is often described as life-changing since it restores vision. And as someone who has always been very near sighted and needed glasses/contacts all my life (and now has presbyopia), that hopefully will be the case with me.
So ... thanks for reading this far and I hope it was helpful/informative to 'ya. Wish me luck! ;-)
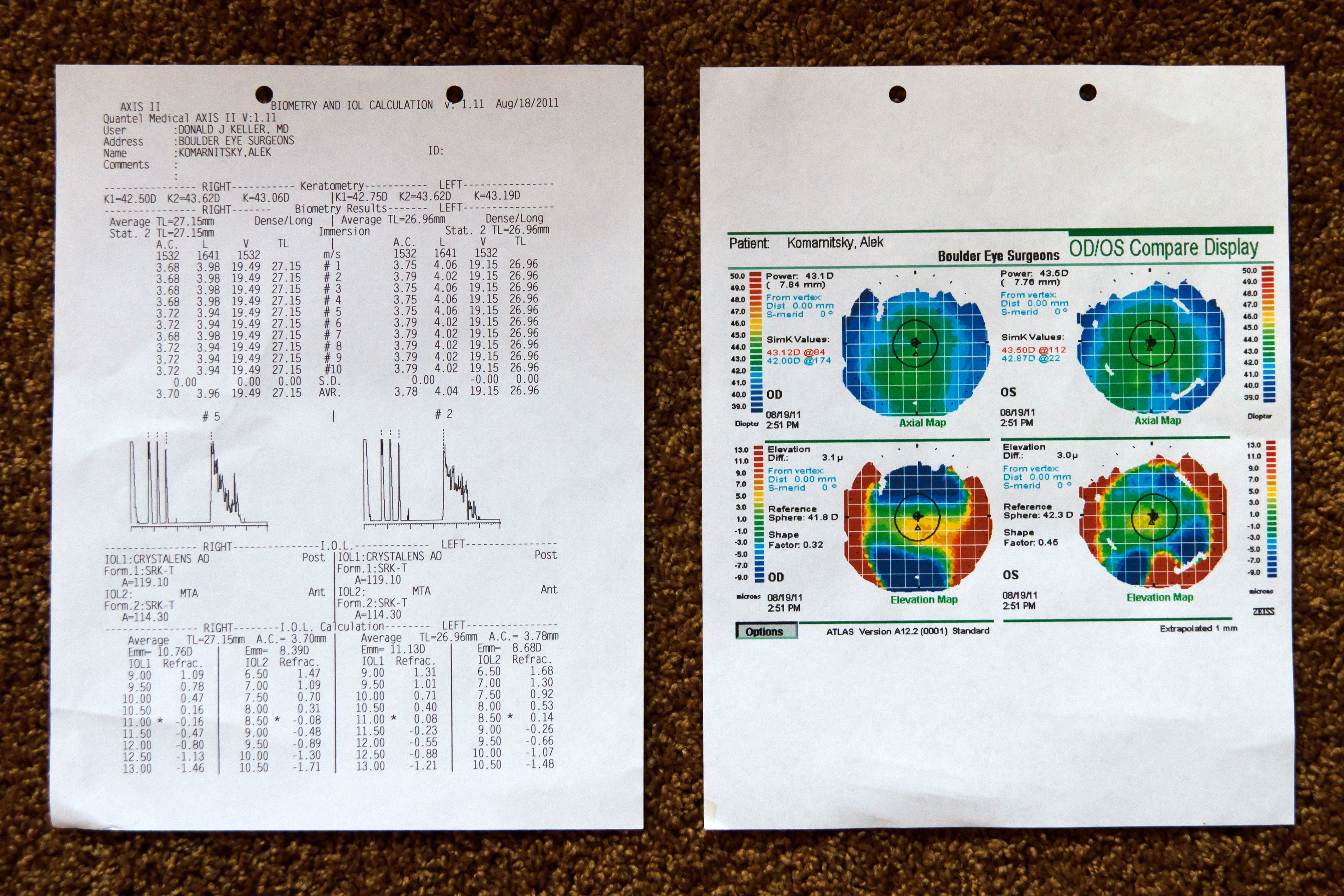
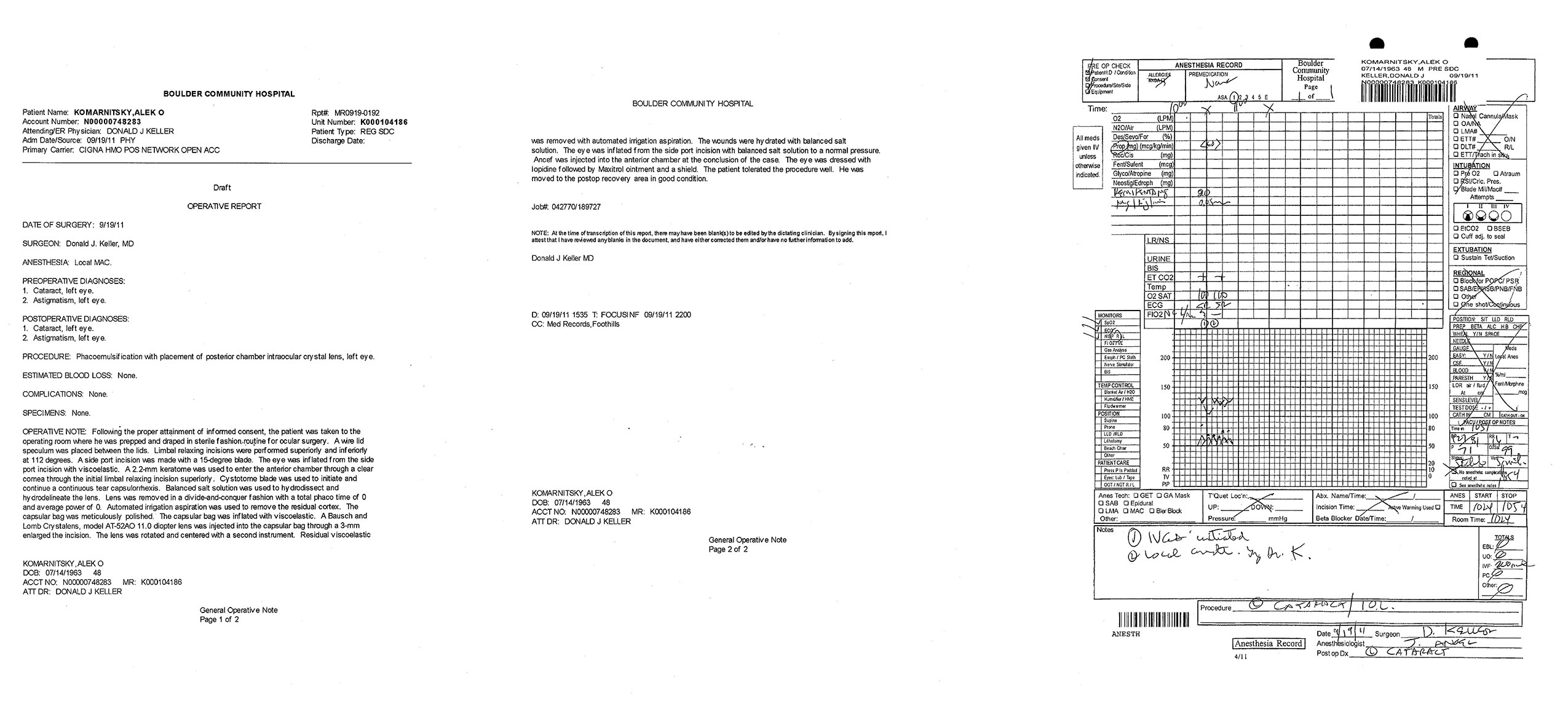
The Corneal Topography showed 1.12 diopters of astigmatism in the right eye and 0.63 in the left, so Dr. Keller will perform Limbel Relaxing Incisions (LRI's) and hopefully reduce most of this. The IOL calculations recommend an 11 Diopter lens in the right eye that will (ideally!) result in a refraction of -0.16. For the left eye, he may slightly under-correct the power to allow for a bit more close-in vision depending on how it goes with the right eye. BTW, my pupil size was ~5mm in a dim examination room.
Biometric information on my eyeballs - click on the image to see in full-res
I'm scheduled to have the right eye done on Monday, September 12th, 2011 and the left eye a week later ... assuming no complications. By happy coincidence, my Mom is visiting Boulder, Colorado then, so for the first operation, it will be nice to have her around to help. BTW, the main reason for doing the two eyes "only" a week apart is that it will be very difficult to live/function with the right eye corrected and the left eye still needing over 7 diopters of correction ... talk about bi-polar vision! Check back after then for a (hopefully positive) update!
{kind=link}
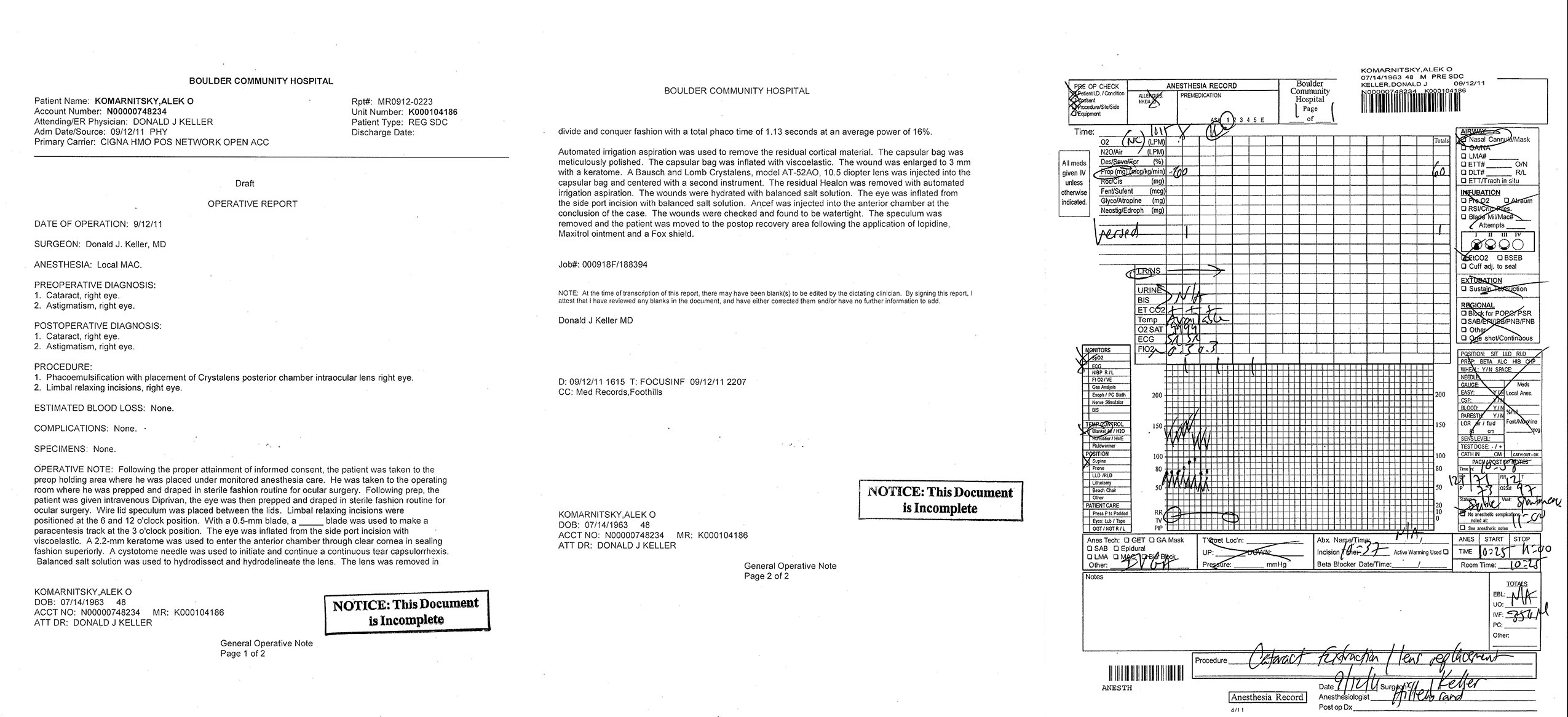
Dr. Keller inserted a Crystalens model AT-52AO 10.5 diopter lens (SN#10-681616) through a 3mm opening - an 1/8" inch! This is slightly less than the 11.0 power "recommended" from the biometry data. He explained that as the eye heals, it usually "pulls back" a 1/4 to 1/2 diopter, so he's hoping the 10.5 will result in me ending up plano - i.e. focus point at infinity when relaxed and hopefully clear 20-20 (or better) vision.
I didn't feel any pain in the eye and the most annoying thing is that the patch is not opaque ... so you have a "white veil" image coming in from the right eye that totally messes up your brain when it combines with a "good" image from the left eye. So I put a "pirate patch" over it to better obscure the right eye which makes it *much* easier to see - too bad it's not Halloween! ;-)
So far, so good ... the patch comes off Tuesday morning and we'll "see" what my vision is like.
I get to wear this colorful hospital patch after the Cataract Surgery - it stays on for a day

Pirate Patch makes it easier to see - too bad it's not Halloween as I could go as a Hulk'in Jack Sparrow! ;-)

This is obviously an excellent sign and after examining my eye, Dr. Keller said everything looked good and healthy and he'd expect some improvement in distance vision by the Friday appointment. I was able to read (barely) 20-40 in an intermediate vision test 24 hours after my surgery, but the accommodation can take several months and you don't want to be over-corrected. Recall I had -7 diopters of myopia so I could focus 5" from my eyeball - knew I'd lose this ability and will miss it. Initial impressions are low-light/night vision is improved. I do see some occasional "shimmering" on bright light sources in my peripheral vision along with a few dark floaters - I believe both are normal.
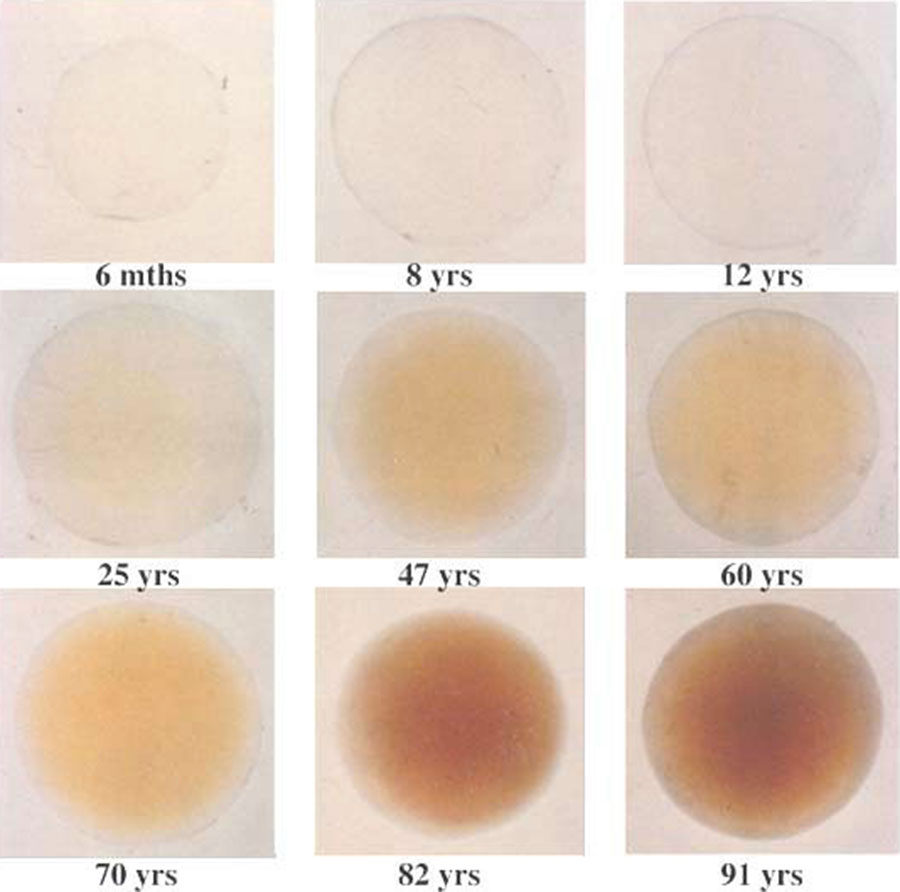
Another thing I have noticed is colors are more vibrant plus generally brighter. This is very common after cataract surgery and is probably due more to the yellowing of the natural lens with age ... which is pretty subtle as it "sneaks" up on you less noticeably than the loss of vision.
The human crystalline lens at various ages from Sidney Lerman's "Radiant Energy and the Eye"
The image below gives an idea of how a cataract shifts colors. I used Photoshop to simulate this by applying a +15 with Selective Color (Yellow/Yellow) and -15 on Brightness. Note that this is based on a direct comparison between my right eye (new lens) and my un-operated left eye (48 year old natural lens) which did not have a vision impairing cataract. I.e. the cataract was surely causing even more dullness - see what it did to Monet!
Image "flip" simulation showing how aging of your natural lens causes yellow hue & dimness - cataract was more!

There are other subtle color shifts and I've also seen a few "big" shifts a handful of times ... which may be due to me seeing some Ultraviolet light that was filtered by my natural lens before ... or maybe I'm just much more sensitive to the bottom of the visible spectrum around 400nm. The shift goes away when I used a camera UV filter. Some info here and another plus an eye surgeon report here and I'd like to test my color vision with a Monochromator. Using an online FM100 Hue test, I scored an 8 (seems pretty good) with the few errors in the green-blue area. I re-took the test (only takes a few minutes) in early/2018 and got none wrong - perfect score!
Here's a picture taken in the shade on a sunny day of my son's Colorado Rockies shorts and other misc.
The camera (and other people) don't see the purple glow - simulated with +20% Red & Blue channel
If I put a UV filter (or a pair of plastic biking glasses) in front of my eyes, the purple glow goes away
Click here to read more details/analysis on the violet glow as seen through a Crystalens

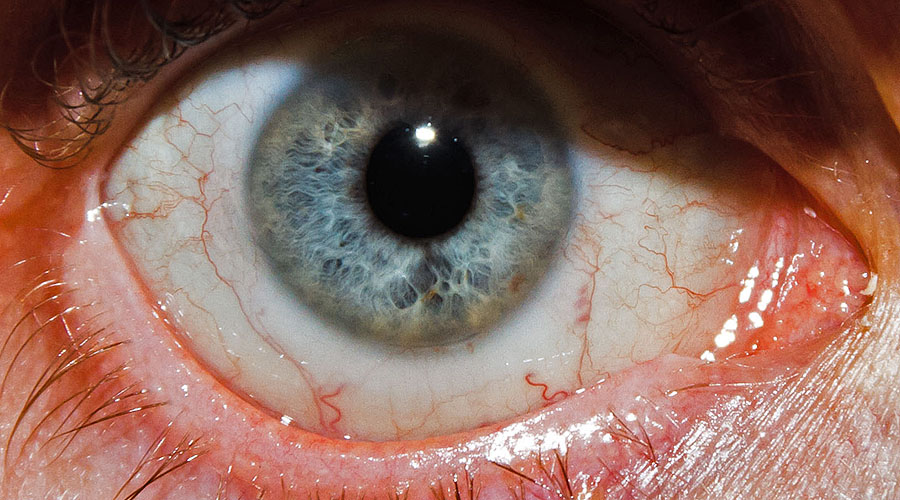
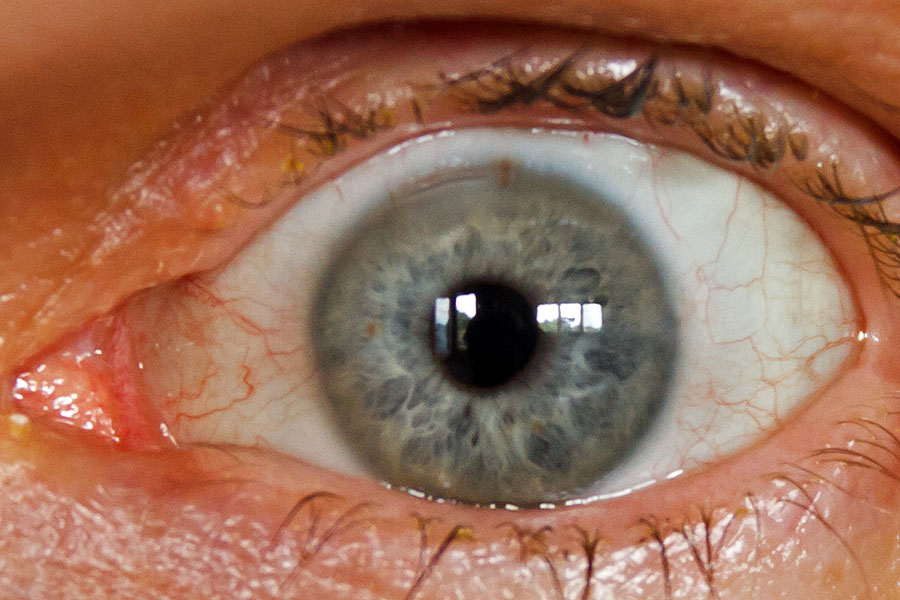
My mom volunteered (!) to take a few closeup pictures of my eyes after the first Cataract Surgery
Note Dr. Don Keller's initials (placed pre-op) next to the right eye

Closeup of right eye - believe that is the Limbel Relaxing Incision (LRI) and entry point at top - click to see lower one
{kind=link}
One challenge is that the right eye is now close to 20-20, but the left eye is still -7 diopters ... so there is a big variance between the images from the two uncorrected eyes. You'd thinking that wearing glasses on the left eye would make it better (so now both are close to 20-20), but in some respects, this makes it more difficult due to the "Coke Bottle Effect" - i.e. the glasses make the image smaller and create distortion at the edges - this is called Aniseikonia and more info. So this is why I want to do the second eye one week after the first rather than wait.
Aniseikonia ("Coke Bottle Effect") flip simulation comparing image as seen by the right eye with no glasses (after cataract surgery and corrected to 20-20) compared to the uncorrected left eye with -7 diopter glasses

The combined image isn't this "bad" in real life, but still quite the challenge for the brain to sort out

Speaking of how the brain processes visual info, here's one of many interesting demos. The areas that "appear" to be blue and green (i.e. different colors) are actually the same color with RGB values of 0,255,150. Look at the closeup merge on the right and bottom.

We debated whether to go with an 11.0 Crystalens or an 11.5. As mentioned earlier, one can "offset" the two eyes so you have better closer vision, but at a loss of distance acuity and depth perception. According to the calculations, the 11.0 in the left eye would be 0.08 diopter more myopic than the 10.5 is in the right eye - the 11.5 would be another 0.31 diopters myopic. My goal is still the same - hoping to have sharp vision at distance with adequate accommodation for intermediate computer work ... and am willing to wear reading glasses for close-in. We decided to go with the 11.0 to match hopefully match the right eye as I would surely "notice" the mono-vision option.
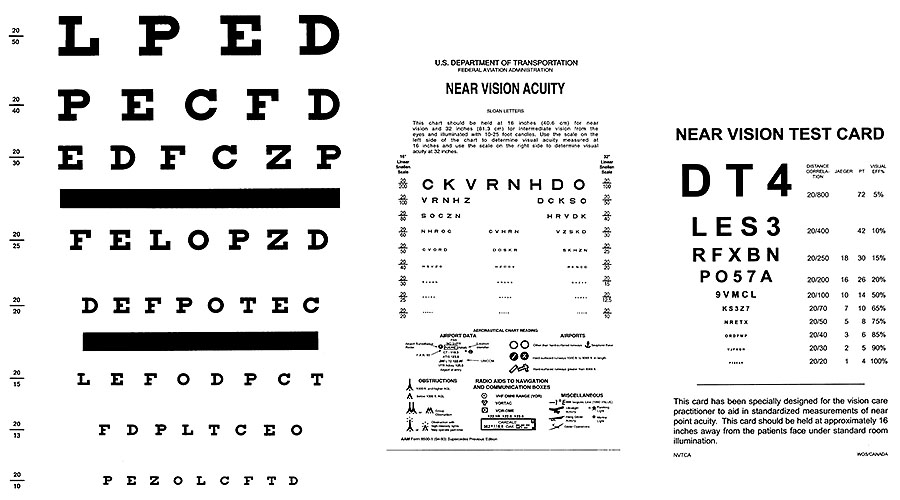
Recall one main reason I selected the Crystalens was for the accommodative ability. Using the FAA Eye charts, I'm seeing 20-20 at distance (not quite as good as measured at the eye doctor), 20-40 at an intermediate range of 32" and 20-100/J10 at close-in range of 16". I'm hoping in the weeks to come to "see" some improvement in those areas. For comparison, while wearing my (distance) glasses on my (un-operated) left eye, I see 20-20 at distance, 20-25 at intermediate, and 20-50/J5 at near ... the accommodation is worse with contacts.
To test my vision, I've been using the FAA Eye charts: Far - Inter/Near - Near ... and Astigmatism

{kind=link}
I have a bit of a "dull ache" in the left eye (more than I remember in the right) but nothing alarming. I was able to "function" around the house (with only one eye of course) and go for an extended walk around the neighborhood with my wife. I again used a "pirate" patch to darken the semi-translucent patch ... so I'm scary looking and can say AYE MATEY! ;-)
So far, so good ... the patch comes off Tuesday morning and we'll "see" what my vision is like.
Right eye correction didn't change much at +1.00/-1.00@145 so (applying half of the cylinder power) I'm slightly Hyperopic (means I "lose" some of the accommodative power) ... but Dr. Keller thinks I might see a quarter/half diopter pull back which would make me plano. With the correction applied via glasses, the 20-15 line was very clear plus I got some letters at 20-10, so my visual system is working well - WOOT! ;-)
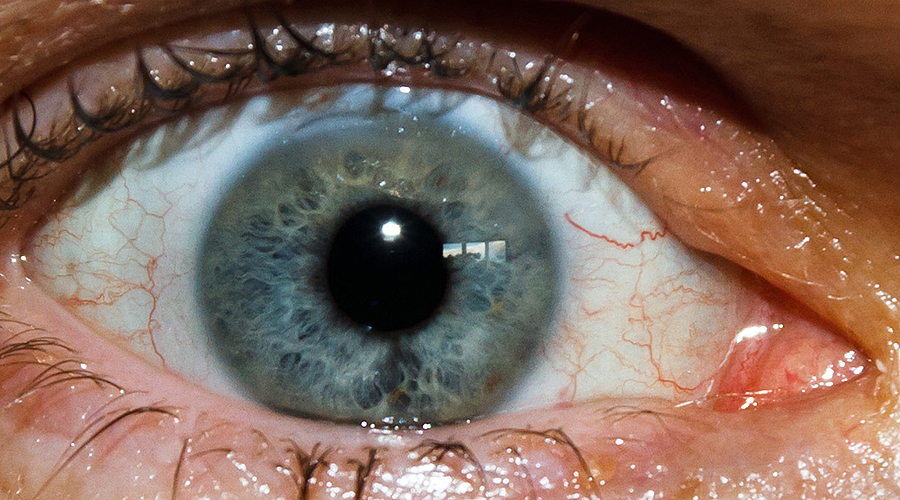
Closeup of the left eye after Cataract Surgery - believe that is the LRI/entry point at top
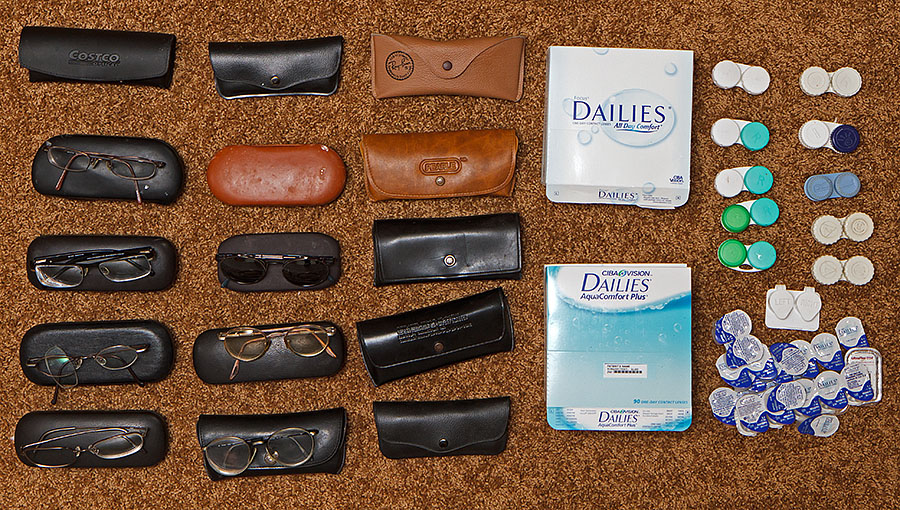
The next day, I gathered up all of my glasses and leftover contacts - there's been countless more over the years
Therapeutic and uplifting to see the pile - will donate the glasses and other misc. and toss the rest - don't need 'em anymore! ;-)
I had some +1.50 reading glasses, but picked up a +1.00 (for $3!) so my eyes will have to work "harder" for intermediate and close-in work. Spent a good part of the day on the computer without glasses, but I get tired after a while ... good exercise/training for the Ciliary muscles! ;-)
The refraction for the right eye didn't change much in the 2nd week ... in fact, she originally got the same +1.00,-1.00@145, but Dr. Keller showed that +0.50,-0.75@145 was very similar. The left eye was 0.00,-0.50@180 after one week, but I feel like it sees less astigmatism. Not perfect numbers, but not too shabby!
I still have occasional shimmering in my eye - typically when a strong light source is at the edge of my vision. This is called pseudophakic photic phenomena or Dysphotopsia and is common in Cataract patients, especially initially. A related phenomena is Negative Dysphotopsia - an occasional dark spot pops up in my peripheral vision. This catches my attention - was that a person (or animal/bird) over there! ;-)
Both are due to the different light paths through the intra-ocular lens (especially the edges) and in many cases, these will go away as the brain figures out they can be filtered away. That's been my experience as I hardly see 'em anymore from the right eye, but still periodically from the left eye, which is one less week post-op. Dr. Keller says a common occurrence that should go away soon ... so I basically just try to ignore 'em.
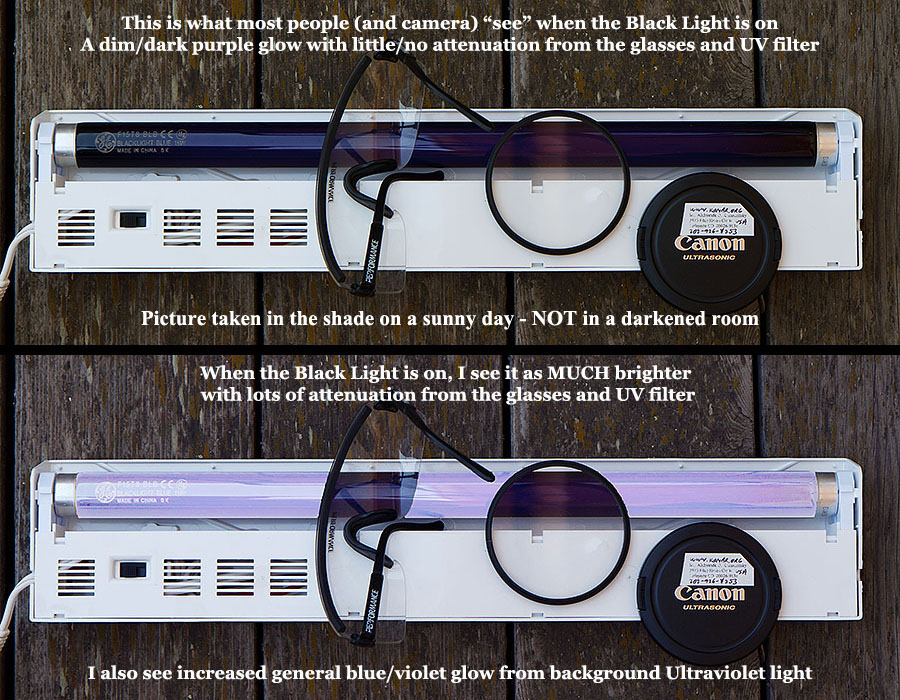
Dr. Keller and I discussed the "violet glow" I mentioned earlier - this is seen equally on both eyes. I stopped by a Halloween store yesterday and when looking at a (fluorescent) black light, it appeared a very bright blue. When I put some poly-carbonate safety glasses on, it went back to being a dim deep purple. Several other adults saw the later with no difference with/without the glasses ... and my 13 year old son only saw a very slight difference with/without the glasses. Medical literature says that the photoreceptors are capable of seeing UV light, but it's typically filtered by the natural lens, especially as it yellows with age. So now that my lens has been removed, I'd consider the test case above fairly conclusive evidence I'm seeing in the UV spectrum. Dr. Keller doesn't have the right gear to test this and has heard this rarely happening with the Crystalens and other IOL's - presumably those that don't filter UV. Read more about the Ultraviolet glow.
Overall, I'm very pleased so far with my Cataract Surgery and Crystalens implants. There's a few oddities (but I'm very analytical), but being able to see sharp (!) without glasses is great and the brightness and vivid color of the world is fantastic to look at.
So while I don't have a "Sixth Sense" that allows me to say "I see dead people" (!), I'm pretty sure I'm seeing Ultraviolet light! ;-)
This unusual side effect gives me a "superpower" so I need a purple cape! Read more analysis of my experience seeing Ultraviolet light.
Simulation of how I see in the Ultraviolet
Captain Ultraviolet to the Rescue - click here if you need a crime-fighter wearing super-cool Blue Blockers!

I continue to try to "train/exercise" my eyes by trying not to wear reading glasses or just the minimum +1.0 power ones ... but it's a challenge to read in low-light conditions - hopefully I'm not just seeing increased depth-of-field in good light. Distant vision continues to be excellent - night driving is soooo much easier with very minimal halo/glare. I still see occasional shimmering (usually if my eyes are dilated and a bright light source is at the periphery of vision) and hardly ever see (especially negative) Dysphotopsia anymore.
It's been great playing some sports recently as I can see the spin of the baseball, arc of the frisbee, and trajectory of the football. A week before my surgery I mountain biked to the top of Rollins Pass and remember how difficult it was to see coming down as my eyes/brain didn't seem to be able to process the distorted/fuzzy imagery as I bounced along. I did some off-trail biking with my younger son today and it was night-n-day difference ... the world is in focus and just stays that way without having to "work" on it. In a similar fashion, stuff such as running around on the frisbee field and driving are much easier - I'm excited to see what it's like snow skiing this winter.
I no longer feel even the occasional "piece-o-sand" in my eyes plus there is minimal dryness. Another interested aspect is that I think (!) I can "hear" the world a bit louder - most notably birds chirping when walking. Perhaps my brain was working so hard pre-op on deciphering my blurry vision that I just didn't hear so well ... or (more probably) I'm just imagining it! ;-)
I still have some old habits such as sometimes reaching under the bed for my glasses when I wake up in the morning - don't need 'em anymore! And if I'm wearing reading glasses and want to focus even closer, I periodically look above the glass, since in the old days, my -7 myopic vision would allow me to focus very close - doesn't work anymore. Another peculiarity is that the world is not only brighter and more vivid, but larger. When I was wearing glasses, the magnification was outside my eye and things appeared smaller - remember my "Coke-Bottle" commentary early. While the image sizes are now matched (thankfully!), I truly do notice that things look a little bigger than I remember them such as golf/ping-pong balls and the moon.
Finally, a number people who have read my writeup (and visual examples) of
seeing ultraviolet light have written to say they see exactly that.
So while I'd still love to do some rigorous testing at an optics laboratory,
I'm pretty darn certain now that I'm truly seeing in the UV spectrum.
I continue to sometimes see purple on grey/black items, but at least so far,
this hasn't been annoying and it's more an interesting oddity.
10/13: My son has a small prism that casts rainbow colors which are well highlighted on the kitchen wall.
I put a yellow sticky where I saw the violet color end, and then asked my wife and kids (age 13 & 10) to show me the "end of the rainbow" ... which was less than I saw ... and about the same as the camera sees.
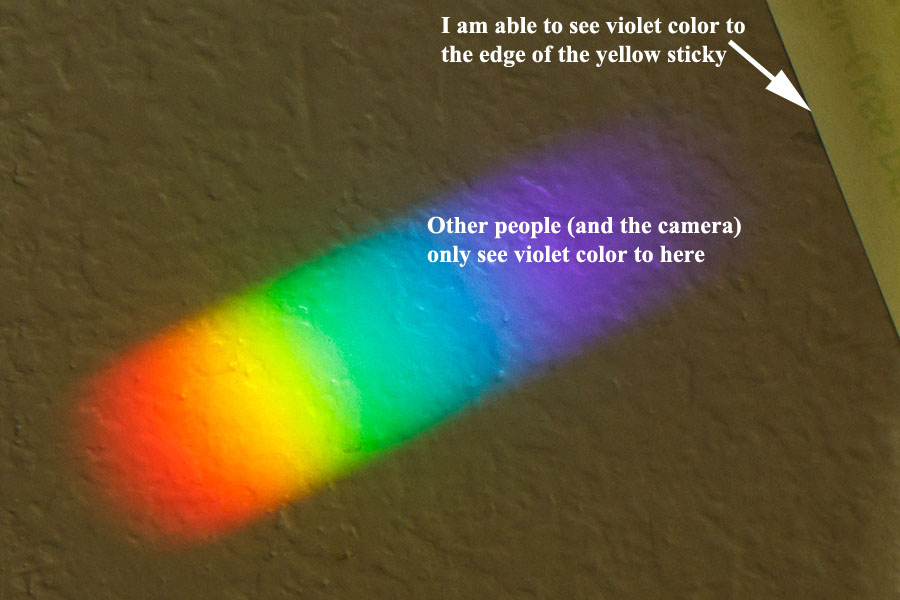
There's more pictures/analysis on the Ultra Violet page but in summary, I was able to see down to 340/350nm ... whereas similar aged people cut-out between 410-430nm. So this seems to conclusively prove that I'm able to see into the Ultraviolet spectrum.
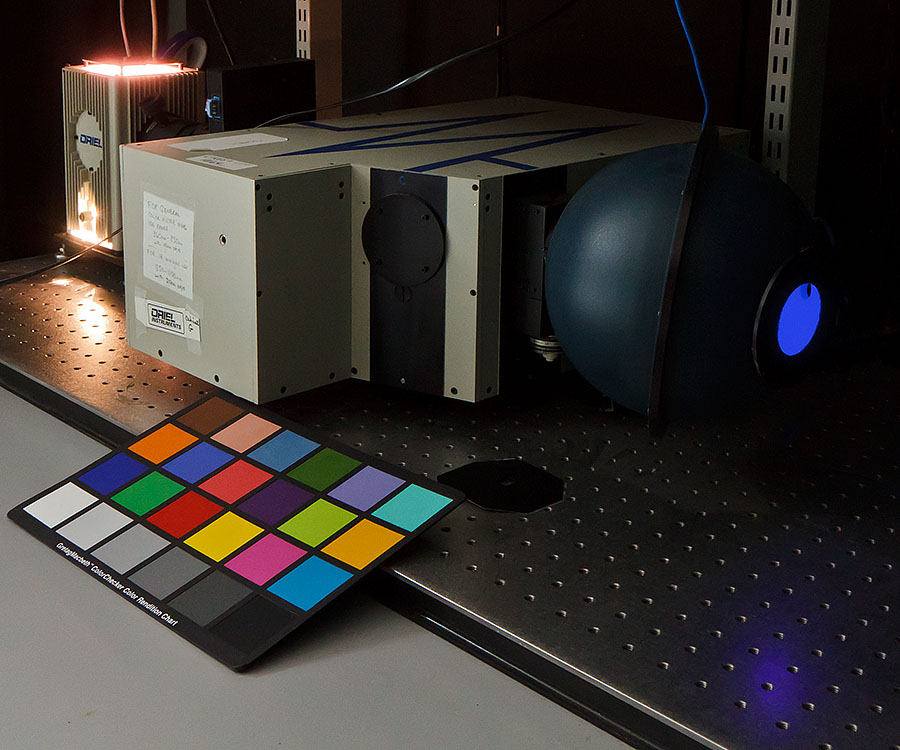
The Oriel Instruments MS 257 Monochromator emitting at 450nm - note massive cooling radiator for source light
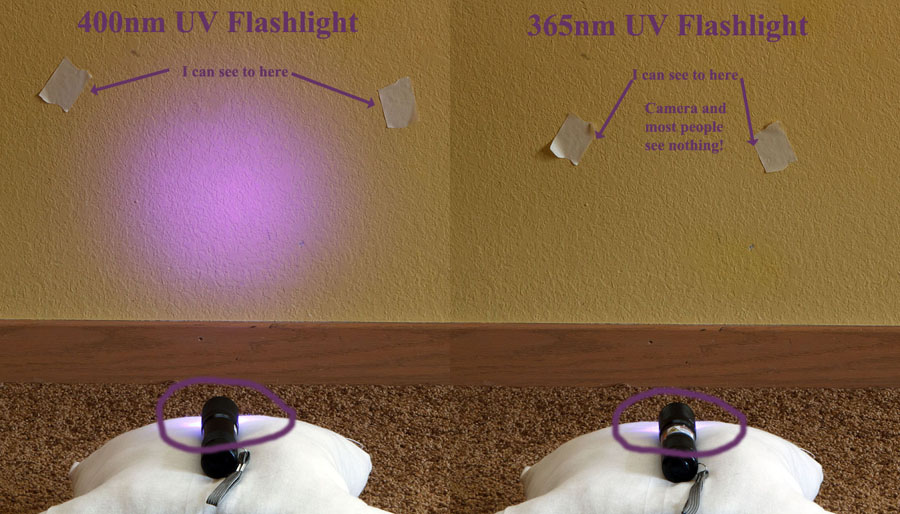
I also picked up 400nm and 365nm UV flashlight to "test" my vision more.
While both have leakage into the visual spectrum
(which starts around 400nm), the 365nm light is a faint/pale grey to "normal" people ... whereas I see a bright purple.
So makes for a very easy demo of my ability to see UV.
Here's a picture of them "lighting" a non-fluorescent wall - remember that the camera doesn't "see" UV.
{kind=link}
In terms of accommodation, the left eye has gotten a bit more, but the right eye has regressed slightly. Both are less capable in the evenings; perhaps the muscles are tired at the end of the day. When looking at the 32" intermediate chart at arm's length (~30") in good light with +1.0 readers, the left eye can read 20-15 and the right 20-20 ... my layman's interpretation is that this is about a 1/2 diopter of accommodation.
Close-up vision in dim light remains a challenge - I need readers to make out the menus at restaurants unless very good light. My son had an eye appointment with Dr. Brain Nichols (Dr. Keller's partner) and he was gracious enough to take a quick look at my non-dilated eyes and said it looked like a slight amount of posterior capsule opacification with a bit more in the right eye ... so it's possible this may be contributing.
Finally, an interesting "visual" while taking an evening walk with my wife tonight as we spotted a Great Horned Owl in a heavily wooded area. With the fading light, it was very difficult to pick him (her?) out as the owl's feathers blended in with the branches. Wendy is an extraordinary wildlife spotter ... and pre-surgery, she pretty much always saw wildlife before me. But in this case, I actually was the first one to pick out where the Owl had landed. I.e. an impressive demonstration of (distance) visual acuity in a cluttered low-contrast, low-light situation.
Back in the 1960's when I was a biology grad student at UCSD, there were reports that a spectroscopist named, IIRC, Gregorio Weber could see UV after cataract surgery too. At the time there was speculation that what he was seeing was not UV directly, but rather the UV-induced fluorescence of pyridine nucleotides and other fluorescent cellular constituents. The result was the same, of course, he could now perceive UV light with his eyes. I suppose the idea could be tested by looking at the action spectrum or by determining is the spatial resolution for UV was the same as for blue light.
That's a good question in terms of the actual mechanism of UV vision ... and I actually have not done any spatial resolution tests which would require an eye test on a chart only seeable in the UV spectrum ... seeing the purple'ish ting on a pair of "black" shorts doesn't count!
It's not a big difference on the eye chart (which is very sensitive to the amount of light) but quite noticeable in my day-to-day routine as I am reaching for reading glasses more often, especially in low light. At night, I struggle a bit to read the newspaper at about 18" away even with +1.5 readers ... which should correct to 1/1.5 meters or 26" ... so I don't seem to be always getting that extra 0.5 diopter of accommodation. I also notice the limited depth-of-focus when the newspaper is on the table since the print is at varying distances. My arms and head seem to be moving things back-n-forth more as the focusing mechanism! ;-)
This may be due to posterior capsule opacification (note comment on March 18th) which I'm hoping is the case since this is semi-expected and should be fixable with a YAG laser. I'll do a formal eye appointment at the one year point and we'll "see" what happens.
He felt the change in the right eye was probably due to some slight scar tissue that may be preventing movement, but otherwise the inside of the eye looked good with some very slight PCO. He also saw some floaters in the right eye, although the left is much more noticeable to me. So no need to do YAG at this point (from a visual point of view) although he did say that people often see a slight improvement in accommodation from this procedure as it can allow the Crystalens to flex more posteriorly.
There was no difference after rinsing the eye with a few drops of saline - just wanted to make certain this is something internal to the eye rather than on the surface. It is completely localized to the right eye and there is no associated pain/feeling - just a slight obscuration of vision that mists over in normal activity due to the "floater" - I did not see any "flashes" of light - another sign of possible retinal detachment.
I was a bit concerned as my risk for vitreous separation (and retinal detachment) is much higher after cataract surgery and especially being highly myopic. Fortunately, Dr. Keller was able to see me the next morning, and after a dilation, he confirmed his suspicion of a posterior vitreous detachment (PVD) in the right eye. These are actually quite common, especially as we age ... and fortunately, I don't have a retinal tear or detachment as these require surgery. Earlier that day, I had a pretty good (accidental) collision while playing Ultimate Frisbee, and getting bumped can cause a PVD.
There is no real treatment for PVD - it eventually heals itself and most symptoms (including hopefully the floater) will go away. Dr. Keller said keep an eye out (pun intended) for an increase in floaters (especially black or red ones), flashes of lights, and the before-mentioned curtain ... as in the short-term, my chance of a retinal tear/detachment increases. However, over the long-term, he said it actually does down after PVD.
On another note, Bausch+Lomb received FDA approval for their astigmatism correcting Crystalens that they call Truelign. This would have been a good choice for me if it had been available in 2011 since despite the LRI's, I have some residual astigmatism.
Happened to noticed that the Skeptics Guide to the Universe did a podcast that talked about my UV vision - here's an excerpt just about that.
Since my corrected vision has been pretty stable, I treated myself with a pair of prescription glasses for both distance and +1.0 Intermediate that also correct for the residual astigmatism and slight over-correction. There's isn't much correction for distance, but they do make things a bit sharper, especially at night ... you can also see that I do better on the eye chart. While I can read the computer screen without glasses, the "+1 readers" really make it sharp ... and easy/faster to read.
The amount of light makes a HUGE difference in how much I can accommodate for closer vision ... although what is actually happening is depth-of-field is increasing as my pupil contracts in light. I can read newspapers/books in sunlight ... but in normal indoor light, like to use at least +1.50 readers to do so.
I continue to get a lot of Emails about my webpage and I'm glad that it has been a helpful resource to so many people. I'm often asked how I'm doing ... and can say that after 3 years, I'm happy with the decision and results. Sure, I wish I had more accommodation ... plus if there was less residual astigmatism, I'd have that extra sharpness. But I analyze my vision more than most and one has to be realistic in their expectations.
Speaking of floaters, the general medical consensus is there isn't much you can do about. Some people are able to "tune 'em out" ... but being an analytical engineer, that unfortunately hasn't worked for me! One possible solution is a Vitrectomy which removes the vitreous humor (and hopefully the floaters) but as with any surgery, it has some risk ... and this is only indicated for severe floaters. Another approach is using a laser to "zap" the floaters, but very few doctors do this - here's a good survey piece by a retired ophthalmic consultant. I've actually had folks Email me about there positive experiences having this done ... so it does appear to work in some cases. Regardless, I have a checkup with Dr. Keller at the end of April, so I'm curious to hear what he sees/recommends after examining my eyeballs.
Oh yeah, and speaking of medical stuff, earlier today I fractured my Fibula snow skiing at Copper Mountain - darn! :-(
I got an interesting Email today from another eye doctor who wrote: "As an eye surgeon who has had a lot of experience using the lens, I found your experience to be pretty normal. Since the average lens power is closer to 20 diopters, the accommodative effect is significantly greater than a weaker lens like 10-11 diopter. [which mine were] Imagine if you were so nearsighted that a zero lens was needed. How much of an accommodative result could you expect with this? None!" That does seem logical, although there may be more to the accommodative effect as suggested by this paper - I could not find much medical literature in this area.
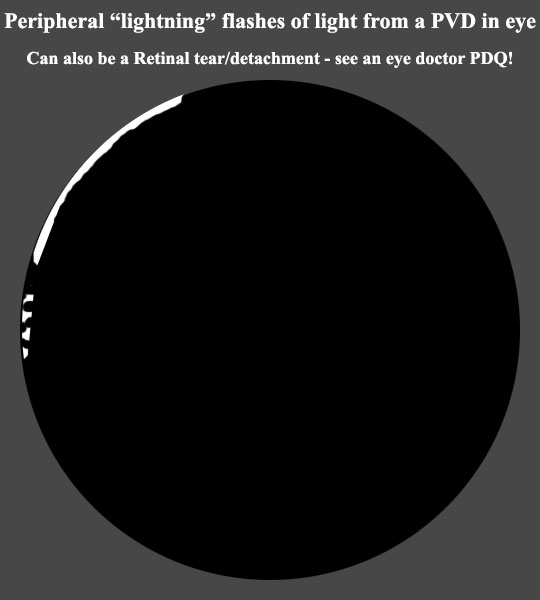
I "saw" these very brief "lightning" flashes every 10-15 minutes, especially if I moved my eye back-n-forth. The pattern was random, but typically a crescent and often some small separated "jaggies" - all on the upper left periphery of my vision. Much less the next morning.
Even though Dr. Keller does surgery on Monday, he was able to squeeze me in and confirmed it is a PVD ... but NOT a retinal tear/detachment. He said good decision to be looked at in case it was ... since if a tear, he would have literally right then, done a quick outpatient retinal laser surgery to seal the tear before it got any worse.
Dr. Keller advised me to take it easy for the next week (hiking OK, but no mountain biking or other impact/head-turning activities) and all should be fine ... but come back if the flashes return. Good news is assuming that the vitreous cleanly detaches, it actually reduces your odds of a retinal tear/detachment.
The main reason I'm writing this update is the blurriness in the right eye has gotten progressively worse - this is almost certainly being caused by Posterior Capsule Opacification (PCO) which commonly happens after cataract surgery. I've been fortunate it has taken this long to develop since my cataract surgery in late/20111. Dr. Keller first flagged it in early/2018 and the visual deterioration become noticeable starting about mid/2019 ... and has been slowly gotten worse.
When I cover up the left eye, my vision is noticeably fuzzier using the right eye at all distances. Applying "plus" near correction doesn't improve distance ... so I haven't gone hyperopic. Fortunately, I don't "see" this too much in normal activities (although binocular vision would be affected) as my brain is using the "good" image from my dominant left eye. But being an OCD Engineer, I notice it probably more than most and find it pretty annoying. BTW, I was kind of surprised that my right eye vision almost goes back to "normal" using a pinhole occluder ... since I would think that the haziness would affect that more.
The fuzziness is more pronounced in high contrast situations and especially bright points of light. The left eye will see it reasonably distinct, whereas the right eye will see a blurry ball around it. Floaters can create a similar visual pattern, but you'll see it change if you move your eyes around as they float in-n-out of the visual path.
So it's time to have the YAG laser surgery to clear it up. This takes just a few minutes (totally outpatient with no anesthesia) and basically is a focused laser that "burns" away the back of the capsular bag so the hazy section falls away and doesn't obscure the optical path - here's a good writeup. While any procedure has some risk, this one is very minimal and should clear up the right eye fuzziness right away ... and since the left eye will also be done, it could also provide better vision there due to a clearer optical path. Note that after the hole is "blasted" in the back of the bag, trying to replace an IOL would be much more difficult ... but ideally that should never have to be done anyway.
Per my October 30th, 2019 update, Dr. Keller said there's a chance of a slight (~+0.25) hyperopic shift (which I hope does not occur) but also that the YAG treatment may "relax" the Crystalens hinges and provide some accommodation - i.e. better near vision. I would be ecstatic if that actually happened ... although realistically, I think the odds are low.
Both eyes are typically done at the same time, so I'm looking forward to next Monday when Dr. Keller will fire a laser at my eyes! ;-)
He then "shot" both of my eyes with the YAG laser to "blast" the PCO. Just before that, I got a drop of 0.5% Apraclonidine (proactively to reduce IOP) and 1% Tropicamide (dilate the eyes) and afterwards another drop of Apraclonidine. The laser itself takes about a minute per eye. The left took 37 shots (each at 1.8 milliJoules) for a total energy of 68 mJ. The right eye (which had more fuzzy vision and Dr. Keller confirmed looked much hazier to him) took 109 shots for a total energy of 198mJ.
One thing I noticed right away was all sorts of floaters in both eyes, which is to be expected ... since Dr. Keller basically blasted a 5mm hole in the back of the capsular bag. It's kind of wild using high powered binoculars to look at the sky (NOT the sun!) and see the pieces floating around. These should dissipate in the next couple of days.
My initial impression (while the eyes were still dilated) is the fuzziness from the right eye was cleared up ... it actually seems sharper at distance than the left. I'll do some testing in the next couple of days to see how I'm seeing at near/intermediate/far and I'm hoping there is minimal hyperopic shift. I have a follow-on appointment with Dr. Keller at the end of the month, so real curious to see the refraction numbers.
FYI that there were no pre-op prep/restrictions and I drove myself home afterwards (wearing sunglasses) with no post-op limitations.
As mentioned, there is the possibility of a hyperopic shift from YAG and I don't really have the ability to measure/infer small amounts of this ... but my guess is that at least so far, that hasn't happened - WOOT! ;-)
This seems to be reinforced by the improvement in my near/intermediate vision. The right eye is without a doubt better from just before YAG - again, not surprising since the hazy section was removed. My initial testing shows both eyes are comparable to several years ago and (maybe!) slightly better. While looking at the intermediate/near vision charts, it seems it will sometimes clear up even better .... which suggests (maybe!) some accommodation is going on. I'm real curious to see if this continues and hopefully improves. Note the visual acuity is dependent on good light, so depth-of-field "accommodation" is playing a significant role.
I noticed right away when I put on my +1 readers (with astigmatic correction) that the computer screen (at a meter intermediate distance) is really sharp and dark - love it! With that correction, I'm getting most of the 20-15 letters on the intermediate chart even in not-so-bright light. Another thing easily noticed is when looking at bright points of light, the "blurry ball" (caused by PCO) is no longer seen from the right eye.
Just for grins, I fired up my 365nm UV flashlight and grabbed a piece of Woods Glass (filters visible light) and a UV filter. When my son looks at the flashlight through the Woods Glass, it goes almost completely dark (he can't see UV) ... whereas I can still see quite a bit from the UV. Putting the UV filter in front of the flashlight (both with/without the Woods Glass) makes very little difference for him (he doesn't see UV) ... whereas for me it's a big difference (since the UV is now being filtered). None of that is surprising - the YAG procedure removed material so if anything, I might see a bit more of the UV spectrum that was being filtered by that. But I don't have adequate tools to evaluate that - would need to do another round of testing with a Monochromator as I did 9 years ago.
For Intermediate, the left eye can see some 20-25 and it's better than before. In fact, I usually wear +1 glasses when using the desktop computer, but I'm much more able to do so without correction now. While it's not as sharp, I figure this is good accommodation "exercise" although it's tempting to put the glasses back on for razor sharp vision. The right eye sees 20-50 and maybe some 20-40. So far, I don't seem bothered by the imbalance and I've tried putting a patch over the left eye to "make" the right eye work "harder" - I don't want it to go "lazy" on me. With pinhole occluder, the left goes to 20-15 and right goes to 20-20 ... man, I wish I had that uncorrected! ;-)
For Near, the left eye will get to 20-50 ... and sometimes 20-40. Again, this is an improvement. The right eye is still struggling and usually is about 20-100 ... but sometimes 20-70. I have to be careful not to squint because both eyes will improve. With the pinhole occluder, the left gets down to 20-20 and right gets to 20-30.
Note that all of the above is in decent light ... so my close-in vision is being "helped" by depth-of-field accommodation. However, I think there is some real accommodation going on ... as my near vision improves if I work on it. When I "work" on the right eye (by covering the left eye), I will every once in a while get a focus improvement ... but have to be careful not to squint which improves both eyes. It's kinda funky to immediately uncover/switch to the left eye (which presumably was trying to focus in sync) and I can read some of the 20-40 line right away.
I continue to have some floaters, but those are decreasing. There are only a few dark spots (looks like fly or gnat out of the corner of your eye) but they are mostly noticeable when I'm doing "eye tests", I'll see some amorphous floaters blur up the vision, but I don't notice it day-to-day. When I look at streetlights at night, there is very minimal glare/haze in both eyes - no more "blurry ball" as seen before with the right eye.
So what this wanna-be-eye doctor make of all that? The laser surgery appears to have been pretty successful. The (annoying) haziness of the right eye is gone and the left eye improved also. The clarity has resulted in better vision at all distances, but the left eye seems to have some "real" accommodation ... it would be awesome if the right eye decided to start flexing ... but I'm probably overly optimistic about that. It also remains to be seen how things change over time.
I see Dr. Keller on October 8th, so I'm curious what a real eye doctor says and what a formal refraction will show.
I mentioned how the left eye seems to have some actual true accommodation whereas the right one does not - he said that is basically the luck of the draw. I'm spending a bit of time "under-powering" my eyes (i.e. no readers or less than normal) with the hope that the IOL will start to flex. I'm not too hopeful, but will give it a shot.
IOP was 18 in both eyes - glaucoma becomes a possible concern if over 21. There is a slightly increased risk of Retinal Detachment from YAG surgery, but the "football" shape of my eyes (remember I was very myopic) would be a bigger reason for that to occur. I'm overall pleased with the results ... although a little more accommodation would have been icing on the cake! ;-)
In summary, it's made out of a UV sensitive material, so after things have "healed/stabilized", the doctor can use UV light to re-shape the lens (multiple times) to adjust it plus/minus 2 diopters of Spherical and 4 diopters of Astigmatism. Note that you *have* to wear UV glasses *always* until you are happy with the results ... at which point it is "burned in." So this not only can fix any refractive surprises, but also allows you to really nail the target endpoint. Here's Dr. Nichol's video presentation with associated slides. It will be interesting to see if this technology fully "works" and becomes commonly used.
My IOP was 20/20 (getting up there - was 18/18 three years ago, but same as last year) and after a thorough (dilated) examination, my eyes looked "very healthy" ... albeit lots of floaters. I forgot to ask about the "half moon pigmentation dropout" in the Supra-Temporal (upper right) of my right eye which was mentioned last year, but presumably it's not there as she did not mention it. So no eye health concerns.
I had them measure my distance (+0.50/-0.50@155 & +.50/0.75@000) and reading (+2.75/-0.75@163 & +2.25/-0.50@179) glasses which I've had for years. Those are still "close enough" that no need to change 'em
My IOP was 22/18 ... so starting to get concerning ... and we "looked" and discussed this quite a bit. Dr. Roa was not concerned as I don't have any significant risk factors ... and my cup-to-disc ratio was 0.25 ... which is considered low. If this was larger (or increasing), that would be an indicator for glaucoma. Plus she said everything looked very healthy. She said I could do an IOP check in 3-6 months, but thought it was unnecessary ... which I agree with.
She did notice (but was not concerned) with what I think was the "half moon pigmentation dropout" in the Supra-Temporal (upper right) of my right eye (seen in 2022), but I forgot it had been flagged before - FAIL by me for not better reviewing my medical history beforehand!
IOP was initially measured using a non-contact tonometer at 15/13 ... which seems abnormally low based on the last 5 years of between 18-22. Dr. Rao used a Goldmann tonometer (the "blue light") and measured 18/18 ... which is more "reasonable" ... and good news is has gone down. Cup-to-Disc ration was 0.3/0.25 ... so that's good also. BTW, those two eyelashes were back ... so even though I hadn't noticed any irritation, she plucked 'em out. I could have them "laser'd" off if this becomes an constant issue ... but we'll hold off on that for now.
My insurance is with Cigna and since Cataract Surgery is a medical condition, they help pay for the operation and a "standard" IOL ... but with a $250 co-pay plus 20%, my out-of-pocket expenses added up to $2,894.90 ... plus $3,700 for the Crystalens upgrade (billed as a markup for the product and the surgeon) for both eyes. So while not cheap, it was less than the $6,000,000 that Steve Austin's bionic eye cost! ;-)
| Item | Billed | Discount | Adjusted | Insurance | Out-of-Pocket | |
|---|---|---|---|---|---|---|
| Anesthesiologist #1 | 630.00 | 210.00 | 420.00 | 336.00 | 84.00 | |
| Anesthesiologist #2 | 540.00 | 180.00 | 360.00 | 288.00 | 72.00 | |
| Eye Surgeon Pre-Op | 280.00 | 85.04 | 194.96 | 154.96 | 40.00 | |
| Eye Surgeon #1 | 2,240.00 | 1,322.25 | 917.75 | 534.20 | 383.55 | |
| Eye Surgeon #2 | 2,240.00 | 1,322.25 | 917.75 | 734.20 | 183.55 | |
| Hospital #1 | 6,902.00 | 2,710.00 | 4,192.00 | 3,153.60 | 1,038.40 | |
| Hospital #2 | 6,318.15 | 2,126.15 | 4,192.00 | 3,153.60 | 1,038.40 | |
| Crystalens Premium x2 | 1,800.00 | 0 | 1,800 | 0 | 1,800.00 | |
| Eye Surgeon Premium x2 | 1,900.00 | 0 | 1,900 | 0 | 1,900.00 | |
| Pre/Post-op Eye Drops | 181.83 | 0 | 181.83 | 126.83 | 55.00 | |
| TOTAL | 23,031.98 | 7,955.69 | 15,076.29 | 8,481.39 | 6,594.90 |
I track my vision with the FAA Eye charts (Far - Inter/Near - Near) and Astigmatism - the eye doctor measuring slightly better numbers.
Note that right eye was done on September 12th, 2011 and the right eye a week later.
| Date | OD - Right Eye | OS - Left Eye | Best Corrected Visual Acuity/Comments | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre-Op | 20-50w/-7.75-1.00@155 | 20-15w/-7.25-1.00@012 | Pre-op numbers are BCVA - needed +2 for reading | ||||||
| +1 Day | 20-20/40/100/J10 | 20-25/40/70/J7 | |||||||
| +1 Week | 20-15-/30-/70-/J7- | 20-15-/30/50/J5 | OD:20-15w/+1.00-1.00@145 | OS:20-15+w/+0.00-0.50@180 | |||||
| +2 Week | 20-15-/30/50-/J5- | 20-15-/30/50/J5 | OD:20-15+w/+0.50-0.75@145 | OS:Not tested | |||||
| +1 Month | 20-15-/30/50/J5 | 20-15-/30/50/J5 | OD:20-10-w/+0.75-1.00@152 | OS:20-10-w/+0.50-0.75@005 | |||||
| +2 Month | 20-15-/30-/50/J5 | 20-15-/30/50-/J5- | |||||||
| +3 Month | 20-15-/40/50-/J5- | 20-15-/30-/50-/J5 | |||||||
| +6 Month | 20-15-/40-/70/J7 | 20-15-/30/50/J5 | |||||||
| +9 Month | 20-15-/40-/70-/J7- | 20-15-/30-/50-/J5- | |||||||
| +12 Months | 20-15-/40-/70-/J7- | 20-15-/30-/50-/J5- | OD:20-10-w/+0.50-0.75@155 | OS:20-10-w/+0.50-0.75@005 | |||||
| +18 Months | 20-15-/40-/70-/J7- | 20-15-/30-/50-/J5- | OD:20-10-w/+0.75-0.50@155 | OS:20-10-w/+0.00-0.50@177 | |||||
| +30 Months | 20-15-/40-/70-/J7- | 20-15-/30-/50-/J5- | OD:20-10-w/+0.75-0.50@147 | OS:20-10-w/+0.50-0.50@177 | |||||
| +3 Years | 20-15-/40-/70-/J7- | 20-15-/30-/50-/J5- | |||||||
| +4 Years | 20-20+/40-/70-/J7- | 20-20+/30-/50-/J5- | OD:20-15+w/+0.50-0.50@145 | OS:20-15+w/+0.25-0.75@002 | |||||
| +5 Years | 20-20+/40-/80/J8 | 20-15/30-/70/J7 | OD:+1.00-0.75@155 | OS:0.50-0.75@005 | |||||
| +6 Years | 20-15-/40-/80/J8 | 20-15-/30-/70/J7 | OD:20-10-w/+0.75-0.75@155 | OS:20-15+w/+0.25-0.50@005 | |||||
| +8 Years | 20-25/50-/100/J10 | 20-20/30-/70/J7 | OD:20-15+w/+0.75-0.50@155 | OS:20-10-w/+0.00-0.75@010 | |||||
| +9 preYAG | 20-40/70-/125/J12 | 20-15-/30-/70/J7 | |||||||
| +9 postYAG | 20-15+/40-/70-/J7 | 20-15/30-/50-/J5 | OD:20-10-w/+1.00-0.75@155 | OS:20-15+w/+0.00-0.25@177 | |||||
| +10 Years | 20-15+/40-/70-/J7 | 20-15/30-/50-/J5 | OD:20-10-w/+0.75-0.75@151 | OS:20-10-w/+0.25-0.50@007 | |||||
| 2022_11_01 | 20-15+/40-/70-/J7 | 20-15/30-/50-/J5 | OD:20-10-w/+0.75-0.75@156 | OS:20-10-w/+0.50-0.50@180 | |||||
| 2023_10_16 | 20-15/50/80/J7- | 20-15/30-/50-/J5 | OD:20-15+w/+1.00-0.75@154 | OS:20-15+w/+0.25-0.25@179 | |||||
| 2024_11_13 | 20-15/50/80/J7- | 20-15/30-/50-/J5 | OD:20-15+w/+1.00-1.00@150 | OS:20-15+w/+0.00-0.50@179 | |||||
| 2025_11_18 | 20-15/50/80/J7- | 20-15/30-/50-/J5 | OD:20-15+w/+1.00-1.00@155 | OS:20-15+w/+0.25-0.75@170 | |||||
A "+" means I got a few letters on the line below and "-" means I missed a few letters on that line.
Tests done consistently with very good indoor light ... so increased depth-of-field helps.
Intermediate/Near vision gets noticeably worse with less light - a bit disappointing not more accommodation.
- While Cataract Surgery is fairly routine these days, there is risk with any surgery - I'm very happy to have had no major complications.
This may actually be a "better" option than Lasik, especially if you are middle-aged and want to try to correct Presbyopia. - Educate yourself on the pro/cons of the various solutions and what you want - I don't believe there is a "best" IOL ... yet.
Along those lines, I really appreciated Dr. Keller's candid comment - "results are limited by limitations in current technology" - You can over-research Cataract Surgery (as I did!), but ultimately you have to trust the eye surgeon who does it.
This sounds good in theory but is realistically difficult as every doctor claims the lowest complication rate, best results, etc. - Be realistic in your visual expectations for far/inter/near and low-light
Especially true if you have any amount of astigmatism - make sure you understand what your surgeon can/can't do about that. - Cataracts "sneak" up on you as the vision slowly degrades, so keep an "eye on your eyes"
The dullness/dimness is subtle (plus your natural lens yellows) and everything looks so much more vivid and bright after surgery. - After seeing my wife go through Breast Cancer Surgery a year earlier, Cataract surgery was a piece of cake in comparison.
I was able to "function" that afternoon and drive the next day - there's little pain/discomfort associated with the process. - Ask the Eye Surgeon/Anesthesiologist if you can stay awake/aware during the operation - it was pretty cool ... for me! ;-)
- If you have significant correction, minimize the time between operations - it's tough have one "good" and one "bad" eye.
Putting a "pirate patch" over the translucent patch really reduces the strain on your brain by producing a dark image. - It's amazing to see 20-20 the very next day, but be patient as there are some visual aberrations that last longer.
- Also have patience (on a longer scale) for the Crystalens accommodation - I'm still waiting/hoping for more, especially in low light.
I don't expect to be able to read without glasses, but one diopter of accommodation would be nice for intermediate viewing at a meter. - While the FDA approval/study had promising results, the Crystalens has fallen out of favor as it seems in most patients, you don't get the hoped-for accommodation.
- Activities that require motion such as sports, driving, etc. are much easier with sharp vision.
- While you won't "see Dead People" (Sixth Sense), you might see Ultraviolet light which is kinda interesting.
- Consider having Cataract Surgery done sooner rather than later - as one MD found out.
I consider myself fortunate to have a fairly successful outcome and "see" the world in a whole new light! ;-)
I hope my longgg writeup was informative and useful - contact me with any corrections/questions/suggestions.
And if this was helpful, there's a link on that page if you want to buy me a beer ... or some Big Mac's! ;-)
Holy cow Alek, there is so much good information in your cataract description.As an engineering manager with a long history in color science, optics, and image processing, I totally geeked out at your descriptions. I've wondered how multifocal lenses work. Now I know. I wondered what the state of IOL's with accommodation were. Now I know. I knew you see more deep blue after cataract surgery, but wondered what that's like. Now I know. I'm 55 and still have 20/20, but when I ask my eye doctors about any of this stuff, they can't explain it nearly as well as you do. I was chuckling the whole way through your cataract diary thinking "I'm blown away by the amount of research Alek did. I'm blown away by all the self-experiments. And I'm blown away that you wrote the whole thing up in so much detail. You're an excellent writer, too."
Thanks for sharing !!!!